

What is cdh?
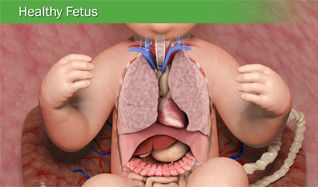

Images used via Children's Memorial Hermann Hospital.
The unfamiliar term "Congenital Diaphragmatic Hernia" is not something any expecting parent wants to hear from their doctor. At first, it's a very odd thing to hear; it sounds strange coming off of your tongue as you explain what it is to other people. Then after awhile, it becomes so a part of your vocabulary that you don't remember life before it.
Congenital Diaphragmatic Hernia (CHD) is a rare birth defect that happens in about 1 and every 2,500 babies in the United States. It is statistically just as common as more well-known defects, like spina bifida and cystic fibrosis. [1] According to research published in the National Library of Medicine by Wynn, Yu, and Chung, Cdh, CDH "account(s) for 8% of all birth defects and 1–2% of infant mortality, making it one of the most prevalent and lethal congenital anomalies." [2] In this defect, the baby's diaphragm does not properly form in the womb early during the pregnancy. This can range from a very tiny hole that eventually only needs a few stitches to fix, or it can be a much larger hole that needs a patch to be fixed. The diaphragm muscle separates the chest cavity from the abdominal cavity. So, when the diaphragm is not formed properly in the womb, the abdominal organs (stomach, liver, spleen, intestines, kidneys) can move up into the chest, overcrowding the heart and lungs. Lungs are the last organs to develop in the womb, which makes this birth defect especially dangerous when babies are born. Two specific lung issues that are most common with CDH are pulmonary hypertension (high blood pressure in the blood vessels of the lung) and pulmonary hypoplasia (abnormally small lungs).
When the baby is born, he/she will have to undergo major surgery within the first few days of life to fix the hernia and move all abdominal organs back into its correct cavity. The baby will need some type of breathing support - this can range anywhere from a nasal cannula, a ventilator, or if the baby is very severe, ECMO.
ECMO (extracorporeal membrane oxygenation) is more or less a life support machine that takes the blood out of the baby's body, runs it through a machine that takes the carbon dioxide out of the blood, and then oxygenates it before flowing it back into the body. Major concerns of a baby being on ECMO include the time frame (baby's cannot stay on ECMO longer than a few weeks before chances of being able to come off drop drastically), clotting (blood leaving the body automatically makes it coagulate), and excessive bleeding (because of coagulation factors, the baby is usually put on a medication called Heparin, which is a blood thinner, and in return risks excessive bleeding). Babies who have CDH have about a 50% chance of survival, and babies who are put on ECMO only have a 50% chance of survival.
Of the babies who do survive, long NICU hospital stays are usually needed. It can be as short as a few weeks, but the severe babies with CDH can take months or a year to recover in the hospital. Long recovery can be from complications of the pulmonary hypertension and/or pulmonary hypoplasia as mentioned above, or from other complications of CDH, such as digestion and feeding problems from gastrointestinal issues.
Currently, the cause of CDH is still unknown.